Finding breast cancer early and getting state-of-the-art cancer treatment are two of the most important strategies for preventing deaths from breast cancer. Breast cancer that’s found early, when it’s small and has not spread, is easier to treat successfully. Getting regular screening tests is the most reliable way to find breast cancer early. The American Cancer Society has screening guidelines for women at average risk of breast cancer, and for those at high risk for breast cancer.
What are screening tests?
Screening refers to tests and exams used to find a disease in people who don’t have any symptoms. Early detectionmeans finding and diagnosing a disease earlier than if you’d waited for symptoms to start.
Breast cancers found during screening exams are more likely to be smaller and less likely to have spread outside the breast. The size of a breast cancer and how far it has spread are some of the most important factors in predicting the prognosis (outlook) of a woman with this disease.
American Cancer Society screening recommendations for women at average breast cancer risk
The COVID-19 pandemic has resulted in many non-emergency procedures being put on hold. This has led to a substantial decline in cancer screening. Health care facilities are providing cancer screening during the pandemic with many safety precautions in place. Learn how you can talk to your doctor and what steps you can take to plan, schedule, and get your regular cancer screenings in Cancer Screening During the COVID-19 Pandemic.
- Women between 40 and 44 have the option to start screening with a mammogram every year.
- Women 45 to 54 should get mammograms every year.
- Women 55 and older can switch to a mammogram every other year, or they can choose to continue yearly mammograms. Screening should continue as long as a woman is in good health and is expected to live at least 10 more years.
- All women should understand what to expect when getting a mammogram for breast cancer screening – what the test can and cannot do.
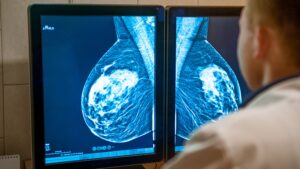
Mammography Screening
Breast mammography is usually performed as a routine health examination. It is an x-ray that takes two or more images of each breast to observe the quality of tissue.
Mammography uses low-dose x-rays to examine your breasts. Our screening centers use digital mammography to capture x-ray images as well as computer images in which the picture can be moved and viewed from different angles.
We also offer digital breast tomosynthesis, which is sometimes called 3-D mammography because it provides a deeper look at the breast tissue.
During a mammogram, you will stand in front of the x-ray machine while the person who takes the x-rays places your breast between two plastic plates. The plates flatten your breast in order to produce a clear picture of the tissue inside.
A screening mammogram usually involves taking two or more x-rays of each breast. The x-ray images can show tumors; they may also show abnormalities that sometimes indicate the presence of breast cancer.
Diagnostic Mammography
Diagnostic mammograms may be performed when a woman (or man) has presented with some type of symptom that requires further examination. This more detailed breast x-ray may obtain additional images to ascertain whether symptoms are rooted in an abnormality such as a breast mass or cancerous tumor. Diagnostic mammography may be performed on patients whose routine mammogram detected abnormalities.
Breast Ultrasound
A breast ultrasound is different than an x-ray. This screening uses high-frequency sonar ultrasound technology to look for abnormalities in tissue. Ultrasound sends sonar waves through the skin into soft tissue. Sound waves “bounce” off masses, resulting in differentiation on the image observed by the sonographer. This test can discern whether a lump is solid or filled with fluid. The ultrasound is often performed at the same appointment as a diagnostic mammogram.
Breast ultrasound (or ultrasonography) uses sound waves to create images of your breast tissue.
During a breast ultrasound, a probe is placed on the skin of your breast. The probe sends high-frequency sound waves into your breast, which bounce off the tissue and return to the probe as echo waves.
The accuracy of the technique depends greatly on the skill level and training of the technician performing it. All technicians at Memorial Sloan Kettering are experts in ultrasound. Currently, we perform this examination if your doctor requests additional screening.
Breast MRI
MRI screenings are more advanced and usually used when a woman has a high risk of breast cancer. Women with breast implants, too, are advised to get MRI screenings, which are more advanced and able to “see” through the implants. Women diagnosed with breast cancer may undergo an MRI to determine the extent and location of tumors.
Breast MRI, when used to screen for breast cancer, involves the use of radio waves and a powerful magnet linked to a computer that creates detailed pictures of your breast.
During an MRI (magnetic resonance imaging) test, fluids are injected to improve the visibility of the inside of the breast.
Studies show that having regular mammography plus breast MRI may offer some advantages over other screening methods for women who are at high risk for the disease. However, it is not typically recommended for women at average risk of breast cancer.
Breast Biopsy
Breast biopsies are usually performed in the doctor’s office. This test may be performed to examine cells for signs of cancer. A biopsy removes a small sample of cells from a mass in the breast. It usually takes just a few minutes, and often includes ultrasound guidance or mammography to locate the abnormality and obtain the most accurate sample.
Breast Tomosynthesis (3-D Mammography)
Breast tomosynthesis, also called 3-D mammography, is a new technology. It takes images of the breast from many different angles and creates a three-dimensional picture of the tissue. Like breast ultrasound, breast tomosynthesis may be particularly useful for women with dense breasts.
Contrast-Enhanced Digital Mammography (CEDM)
Clinical Breast Exam
A clinical breast exam is a physical exam of the breast performed by a trained healthcare professional. It includes an examination of both breasts, your underarms, and your collarbone area to check for any signs of breast cancer.
Breast Self-Exam
A breast self-exam, which you may also call a self breast exam, is an at-home breast exam you give yourself. You’ll want to check your breasts for anything that feels unusual. You should look for breast lumps, changes in size or shape, leaking of fluid from the nipples, or irregular thickening of tissue.
While MSK’s experts recommend breast self-exams for women, they are not a substitute for the routine breast cancer screenings performed by trained healthcare professionals.
Breast Exams at Memorial Sloan Kettering
At Memorial Sloan Kettering, breast cancer screening exams are performed by a team of experts, including radiologists whose sole focus is interpreting the results of breast cancer imaging tests. We offer breast cancer screening services, including mammography, at our Evelyn H. Lauder Breast Center in Manhattan.
We also offer specialized screening services for those at increased risk of breast cancer through our RISE program, available in Manhattan and in New Jersey.
2D vs. 3D mammograms
In recent years, a newer type of mammogram called digital breast tomosynthesis (commonly known as three-dimensional [3D] mammography) has become much more common, although it’s not available in all breast imaging centers.
Many studies have found that 3D mammography appears to lower the chance of being called back after screening for follow-up testing. It also appears to find more cancers, and several studies have shown it can be helpful in women with more dense breasts. A large study is now in progress to better compare outcomes between 3D mammograms and standard (2D) mammograms.
The American Cancer Society (ACS) breast cancer screening guidelines consider having had either a 2D or 3D mammogram as being in line with current screening recommendations. The ACS also believes that women should be able to choose between 2D and 3D mammography if they or their doctor believes one would be more appropriate, and that out-of-pocket costs should not be a barrier to having either one.
Clinical breast exam (CBE) and breast self-exam (BSE)
Research has not shown a clear benefit of regular physical exams done by either a health professional (clinical exams) or by women themselves . There is very little evidence that these tests help find cancer early when women also get screening mammograms.
In some situations, particularly for women at higher-than-average risk, for example, health care providers may still offer clinical exams, along with providing counseling about risk and early detection. And some women might still be more comfortable doing regular self-exams as a way to keep track of how their breasts look and feel. But it’s important to understand that there is very little evidence that doing these exams routinely is helpful for women at average risk of cancer.
American Cancer Society screening recommendations for women at high risk
Women who are at high risk for breast cancer based on certain factors should get a breast MRI and a mammogram every year, typically starting at age 30. This includes women who:
- Have a lifetime risk of cancer of about 20% to 25% or greater, according to risk assessment tools that are based mainly on family history (see below)
- Have a known BRCA1 or BRCA2 gene mutation (based on having had genetic testing)
- Have a first-degree relative (parent, brother, sister, or child) with a BRCA1 or BRCA2 gene mutation, and have not had genetic testing themselves
- Had radiation therapy to the chest when they were between the ages of 10 and 30 years
- Have Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or have first-degree relatives with one of these syndromes
The American Cancer Society recommends against MRI screening for women whose lifetime risk of cancer is less than 15%.
There’s not enough evidence to make a recommendation for or against yearly MRI screening for women who have a higher lifetime risk based on certain factors, such as:
- Having a personal history of cancer, ductal carcinoma in situ (DCIS), lobular carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), or atypical lobular hyperplasia (ALH)
- Having “extremely” or “heterogeneously” dense breasts as seen on a mammogram
This is because although an MRI is more likely to find cancer than a mammogram, it may still miss some cancers that a mammogram would find.
Most women at high risk should begin screening with MRI and mammograms when they are 30 and continue for as long as they are in good health.
Tools used to assess breast cancer risk
Several risk assessment tools can help health professionals estimate a woman’s cancer risk. These tools give rough estimates of cancer risk, based on different combinations of risk factors and different data sets.
Because each of these tools uses different factors to estimate risk, they might give different risk estimates for the same woman. A women’s risk estimates can also change over time.
Who has breast screening?
Each year more than 2 million women have cancer screening in the UK. The NHS Screening Programme invites all women from the age of 50 to 70 for screening every 3 years. This means that some people may not have their first screening mammogram until they are 52 or 53 years.
In some parts of England, the screening programme has been inviting women from 47 to 73 years old as part of a trial.
If you are older than 70, you can still have screening every 3 years but you won’t automatically be invited. To make an appointment, talk to your GP or your local screening unit.
If you are younger than 50, your risk of it is generally very low. Mammograms are more difficult to read in younger women because their breast tissue is denser. So the patterns on the mammogram don’t show up as well. There is little evidence to show that regular mammograms for women below the screening age would reduce deaths from cancer.
it is also for some trans or non-binary people. Talk to your GP or Gender Identity Clinic about this.
After breast screening
You should get your results within 2 weeks. The radiographer can tell you when to expect yours. Most women have a normal reading.
If you have a normal result
You will receive a letter to let you know your mammogram does not show any signs of cancer. Your next screening appointment will be in 3 years’ time. Do contact your GP or local screening unit if you haven’t received an appointment and think you are due one.
It is important to see your GP If you notice any symptoms between your screening mammograms.
If the results aren’t clear
If the x-ray isn’t clear enough or shows any abnormal areas. the clinic staff will call you back for more tests. You might need to have the x-rays taken again.
Risks of breast screening

Although it can find many cancers early, it isn’t perfect. There are some risks, and some people may have a false positive or false negative result.
What is a false negative result?
Screening doesn’t always find a cancer that is there.
What is a false positive result?
In some women, the test picks up something even though they don’t have it. Overdiagnosis and overtreatment
As well as finding cancers that need treating, screening can also pick up cancers that won’t ever cause any problems.
At the moment it isn’t possible to know whether a cancer will grow quickly and need treatment. or will grow slowly, or not at all. So, almost all women diagnosed have surgery to remove the cancer. Many also have radiotherapy, hormone therapy or chemotherapy.
For some women the treatment is unnecessary but at the moment doctors can’t tell who needs treatment and who doesn’t.
Screening can also pick up changes in the lining of the ducts called ductal carcinoma in situ (DCIS). It isn’t possible to tell whether DCIS will develop into a cancer or not. So, many women with DCIS also have surgery and radiotherapy or hormone therapy.
What happens if I have breast implants?
A mammogram is still the best way to detect early cancer, even if you have implants.
This means that it is not as easy to see all the tissue, and you may have more x rays taken. This will help the doctor see as much of the tissue as possible.
It is useful to let the screening unit staff know that you have implants before your mammogram.
Screening for women at higher risk
You can have screening from a younger age if you have a higher than average risk of cancer. This might be due to a family history or an inherited faulty gene.
Speak to your GP if you think you might be at increased risk. They can refer you to a genetic specialist, who can assess your risk. Not everyone with a family history of cancer is at increased risk themselves.
If you have a family history of breast cancer
UK guidelines recommend that women with a moderate or high risk of cancer because of their family history should start having screening mammograms every year in their forties.
If you have a gene mutation
If you have had tests that showed a change in a gene (mutation) that increases the risk of cancer. the recommendations are slightly different.
UK guidelines recommend yearly MRI scans from:
- age 20 for women with a TP53 mutation
- age 30 for women with a BRCA1 or BRCA2 mutation
What is a false negative result?
Screening doesn't always find a cancer that is there. So some people with cancer will be missed. This is called a false negative result.
What is a false positive result?
In some women, the test picks up something even though they don't have cancer. This is called a false positive result and can lead to anxiety and further tests such as a biopsy.




")
{kind=link}
{kind=link}
{kind=link}
{kind=link}